In terms of the constant purchasing power of health care, today's per capita spending on personal health care is 9.2 times as large as in 1929—an annual increase of 2.8 percent. Although the PCE denotes spending by individuals and households excluding goods and services used by government and business, PHCE reflects all spending on health services, including those paid by government and business.
Recall that PHCE excludes current investment in research, new construction, and equipment because their payoffs occur in the future and last more than one year. Realistically, some of the annualized costs of past investments are embedded in the prices paid to medical providers—reflecting funds borrowed to make such investments or funding of depreciation to finance replacement of aging plants and equipment. However, even these costs are understated if they were publicly subsidized.
That said, the measured total of PHCE is the best indication of the extent to which the output of the health sector contributes to the satisfaction of the wants of millions of individuals for medical services. However, PHCE surely is a lower bound on annual expenditures whose motivation is to improve health. For many other purchases (for example, food or even automobiles), health and safety considerations can play an important role. In contrast, PHCE-related purchases typically are motivated solely by considerations of health: Patients do not rely on ambulances to commute to work, nor do they seek a doctor's care to satisfy an empty stomach.
On a per capita basis, real PHCE (that is, inflation-adjusted using the GDP price deflator) has grown over the last 80 years at an annualized rate of 4.1 percent. This implies a doubling of real PHCE every 18 years. Whereas real GDP per capita was approximately 5.3 times as large in 2009 as in 1929, real PHCE per capita grew 24-fold during the same period (figure 2.2). Thus, in terms of what can be purchased in the rest of the economy, PHCE grew more than four times as fast as output.
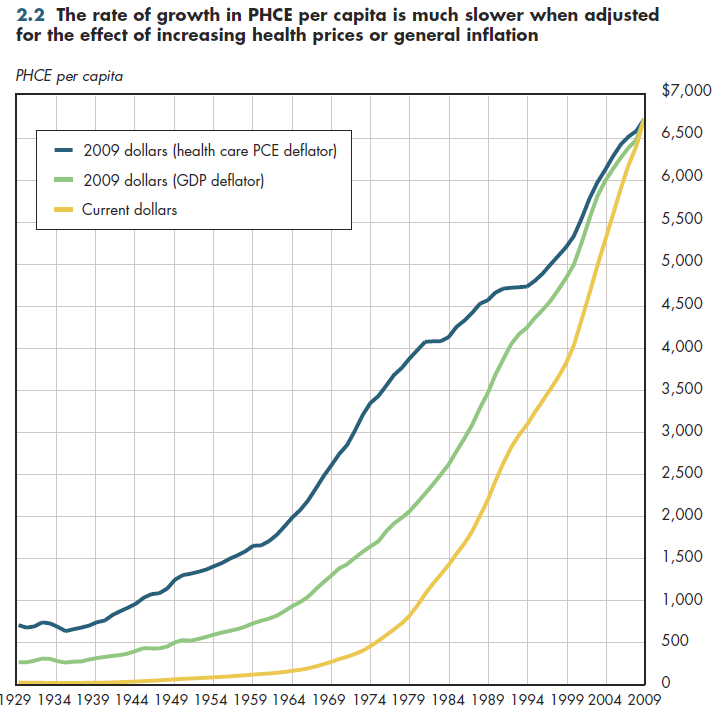
Because health prices have gone up much faster than general prices, this is not the same as saying that real resources devoted to PHCE have grown at that rate. Using the PCE deflator for health care to adjust for prices, today's real per capita PHCE is "only" 9.2 times as large as in 1929.
Download Excel table used to create figure:
Figure 2.2 Table.
Figure 2.2 was created from the following table (the workbook includes all supporting tables used to create this table):
- Table 2.2. U.S. National Health Expenditures by Type of Expenditure: 1929 to 2021
Download PowerPoint versions of both figures.
- Department of Commerce. Bureau of Economic Analysis.
- Department of Commerce. Bureau of the Census.
- Department of Health and Human Services. Centers for Medicare and Medicaid Services.
- Worthington NL. National Health Expenditures, Calendar Years 1929-73. Research and Statistics Note No 1. Office of Research and Statistics 1975.