
Download PowerPoint versions of both figures.
Navigation
-
Lenses
This content is ...
Affiliated with (What does "Affiliated with" mean?)
-
Recently Viewed

- This feature requires Javascript to be enabled.
Inside Collection (Textbook): Chapter 19: Do Americans Get Good Value for Money in Health Care?
19.2 Geographic Differences in Broad Health Outcomes Are Associated with Health Spending
Summary: Geographic differences in broad health outcomes generally are associated with higher health spending, both across countries and within the United States. Because higher spending also is associated with higher incomes, it is difficult to untangle the separate contribution of higher income to better health.
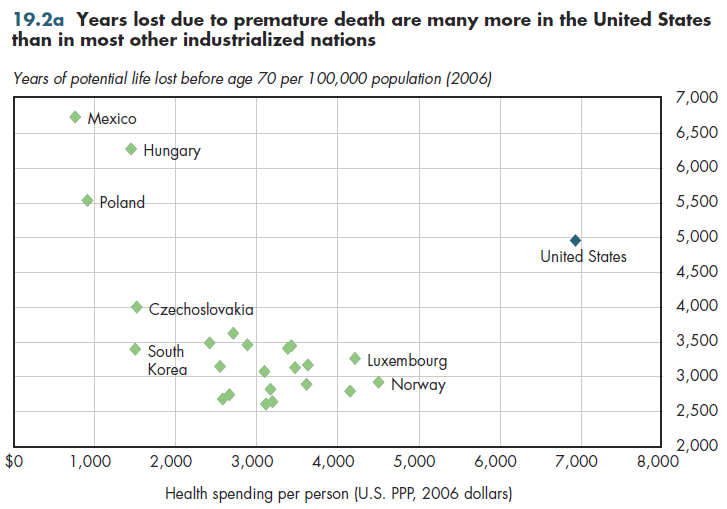
Among industrialized nations, some association exists between expenditures on health and better health outcomes. One approximate cross-national measure of health outcomes is the number of years lost due to premature death. Because life expectancy in industrialized countries now exceeds 70 years, deaths before age 70 are premature. Using this metric, someone dying at age 20 would have lost 50 years of life, whereas someone dying at age 69 would have lost only one year. Giving much greater weight to deaths occurring early in life seems superior to treating all deaths equally. Adding all the years of lost life at all ages and dividing by population numbers provides a standardized measure across countries of different sizes.
Using such a measure, the burden from premature death appears to decline with increased health spending (figure 19.2a). The United States is a rather extreme outlier. It spends much more money on health care but performs much worse on this metric. Some use numbers such as these to argue that the United States does not get good value for the money compared with that of other countries.
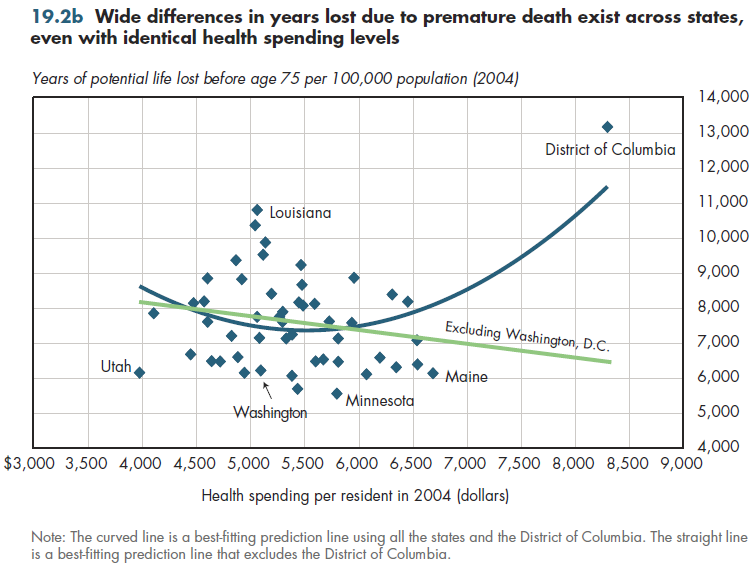
Data from the United States illustrate the limitations of such conclusions (figure 19.2b). First, for any given level of health spending, there is almost a two-to-one difference in the premature death burden. Thus, the huge difference between Louisiana and Washington cannot be attributed to health spending because both states spend almost identical amounts. Conversely, Utah and Maine have almost identical premature death burdens, yet Maine spends almost 75 percent more on health care per resident. Washington, D.C. is an outlier to approximately the same extent that the United States is among industrialized countries. If health spending determined health outcomes, these data would imply worse outcomes with higher spending. Removing D.C.'s unique experience, health outcomes tend to improve with increasing health spending, but other factors clearly make a difference.
Downloads
References
- Author's calculations.
- Department of Health and Human Services. Centers for Disease Control and Prevention.
- Department of Health and Human Services. Centers for Medicare and Medicaid Services.
- Organisation for Economic Co-operation and Development.
Collection Navigation
- « Previous module in collection 19.1 US Health Spending Appears to Provide Good Value for the Money
- Collection home: Chapter 19: Do Americans Get Good Value for Money in Health Care?
- Next module in collection » 19.3 Medicare Spending & Spending Growth Vary Substantially across Geographical Areas
Content actions
Give feedback:
Download:
Add:
Reuse / Edit:
Footer


More about this module: Metadata | Downloads | Version History
This work is licensed by Christopher Conover under a Attribution (CC-BY 3.0), and is an Open Educational Resource.
Last edited by Jia Yao on Sep 24, 2013 3:28 pm -0500.
Twin Cities Campus:
- © 2012 Regents of the University of Minnesota. All rights reserved.
- The University of Minnesota is an equal opportunity educator and employer. Privacy
- Last modified on Sep 24, 2013 3:28 pm -0500