
Download PowerPoint versions of both figures.
Navigation
-
Lenses
This content is ...
Affiliated with (What does "Affiliated with" mean?)
-
Recently Viewed

- This feature requires Javascript to be enabled.
19.9 US Leads the World in Life Expectancy
Summary: Excluding deaths due to violence, the United States generally leads the world in life expectancy at birth.
When life expectancy figures are appropriately adjusted, the United States ranks number one in the world in life expectancy at birth (figure 19.9a). Without such adjustment, the United States ranks fifteenth. The disproportionate number of U.S. deaths due to violence is the principal reason for the nation to rank so low overall. These fatalities include all gunshot-related deaths (homicides and suicides) and also deaths due to automobile accidents or other injuries. Such deaths arguably have little to do with medical system performance but instead arise from social causes, lifestyle choices, or imperfections in other public efforts to reduce such deaths, such as highway safety.
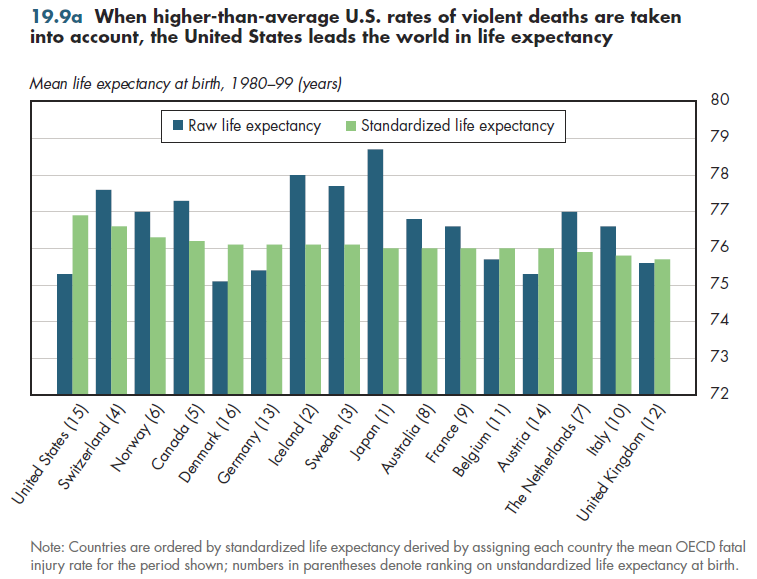
In figure 19.9a, each country was assumed to have the average fatal injury rate experienced over the 20 years examined. This has the effect of increasing life expectancy in countries that have a higher-than-average fatal injury rate, such as the United States. Conversely, it has the effect of lowering life expectancy in countries that have a lower-than-average fatal injury rate, such as Switzerland.
An OECD study shows that the availability of medical care (for example, supply of doctors and nurses relative to the population) is a relatively minor contributor to life expectancy. Increasing GDP per person by 10 percent, for example, would have almost four times as much impact on male life expectancy at birth as increasing the supply of doctors and nurses by the same percentage (figure 19.9b). In addition, increasing the level of education by 10 percent would have at least two to three times the impact as would the equivalent percent increase in doctor and nurse supply.
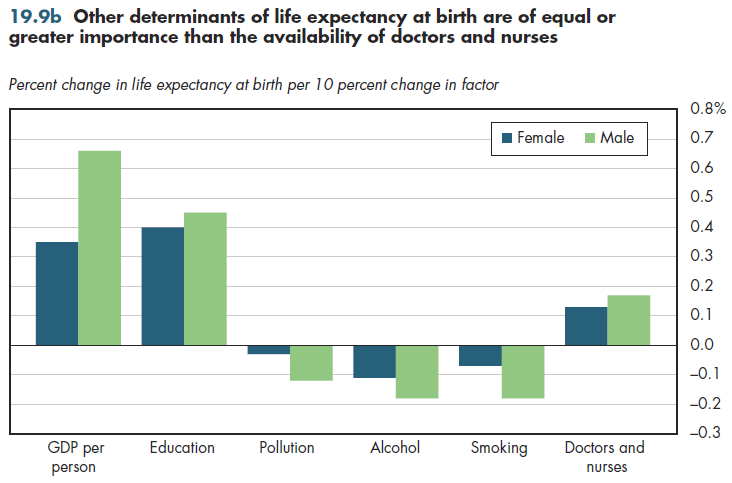
Changing behavior also can produce life expectancy gains that rival an increased supply of medical care services. A 10 percent reduction in smoking or excess use of alcohol (including any use of alcohol resulting in a fatal injury) would produce greater gains in male life expectancy than a 10 percent increase in the supply of doctors and nurses would.
None of these comparisons demonstrates which approach to increasing life expectancy is most cost-effective. They simply illustrate that differences in life expectancy across countries or states could arise even if they have medical care systems that are identical in performance.
Downloads
References
- Organisation for Economic Co-operation and Development.
Content actions
Give feedback:
Add module to:
Reuse / Edit:
Footer


More about this module: Metadata | Downloads | Version History
This work is licensed by Christopher Conover under a Attribution (CC-BY 3.0), and is an Open Educational Resource.
Last edited by Jia Yao on Sep 24, 2013 3:43 pm -0500.
Twin Cities Campus:
- © 2012 Regents of the University of Minnesota. All rights reserved.
- The University of Minnesota is an equal opportunity educator and employer. Privacy
- Last modified on Sep 24, 2013 3:43 pm -0500